A 7-years-aged child was brought by the parents to pediatric OPD with the complaints of on and off swelling of the body (anasarca) for 6 months, and with scrotal swelling, cold, cough, and fever for four days. He had history of frothy micturition for 3 days. He was initially treated at a hospital and was diagnosed to have bilateral Hydrocele and minimal Ascites.
Physical Examination revealed that child was alert, febrile, and with facial puffiness and pedal edema. Urine output was less than 30 mL/day; Weight was 22 kg on admission.
Abdominal Examination on arrival: child had abdominal distension 31cms and scrotal edema

What should be the next step?
Data- Urine protein: 3941 mg/L
- Protein/Creatinine Ratio = 25.6
- Urine Creatinine – 153.6 mg/L
- Albumin +++
- Acetone – Trace
- Bile Pigment ++
- Pus Cell = 6-8/hpf
Histopathology shows normal architecture and there are no significant findings in immunofluorescence as well. What would you do next
Oh ho.. Electron microscopy is never a feasible option in such cases.. Electron microscopy is reserved for cases where no differentials are possible and thus as a final resort we need to look at the biopsy sample through an electron microscope. The parents are vrey upset with the extremely high costs associated with their child’s treatment. They admit their child under a different pediatrician and you are now out of business.
You scored 0 points.
Thank you for completing the case!
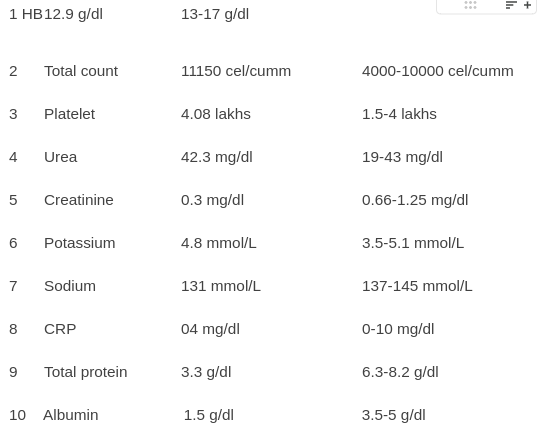
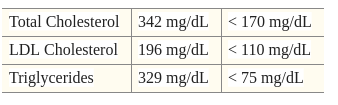
KFT/CBC/Serum Albumin Reports are given.
What’s the next step?
What should be the next step?
Data- Urine protein: 3941 mg/L
- Protein/Creatinine Ratio = 25.6
- Urine Creatinine – 153.6 mg/L
- Albumin +++
- Acetone – Trace
- Bile Pigment ++
- Pus Cell = 6-8/hpf
What’s the next step?
USG reveals mild ascites, mild pleural effusion, edematous gall bladder wall, bilateral normal kidney with raised renal cortical echogenicity
What’s the next step?
KFT/CBC/Serum Albumin Reports are given.
What’s the next step?
USG reveals mild ascites, mild pleural effusion, edematous gall bladder wall, bilateral normal kidney with raised renal cortical echogenicity
What’s the next step?
What should be the next step?
Data- Urine protein: 3941 mg/L
- Protein/Creatinine Ratio = 25.6
- Urine Creatinine – 153.6 mg/L
- Albumin +++
- Acetone – Trace
- Bile Pigment ++
- Pus Cell = 6-8/hpf
KFT/CBC/Serum Albumin Reports are given. What’s the next step?
KFT/CBC/Serum Albumin Reports are given. What’s the next step?
What should be the next step?
Data- Urine protein: 3941 mg/L
- Protein/Creatinine Ratio = 25.6
- Urine Creatinine – 153.6 mg/L
- Albumin +++
- Acetone – Trace
- Bile Pigment ++
- Pus Cell = 6-8/hpf
What’s the next step?
KFT/CBC/Serum Albumin Reports are given. What’s the next step?
What’s the next step?
What should be the next step?
Data- Urine protein: 3941 mg/L
- Protein/Creatinine Ratio = 25.6
- Urine Creatinine – 153.6 mg/L
- Albumin +++
- Acetone – Trace
- Bile Pigment ++
- Pus Cell = 6-8/hpf
KFT/CBC/Serum Albumin Reports are given. What’s the next step?
What’s the next step?
USG reveals mild ascites, mild pleural effusion, edematous gall bladder wall, bilateral normal kidney with raised renal cortical echogenicity
Using Furosemide to treat mild ascites and pleural effusion that did not cause any symptoms lead to the patient ending up in mild dehydration. How would you manage the patient now and what are the steps to be taken next?
Administering IV fluids when not necessary, lead to the child’s parents getting upset about the quality of treatment at your hospital and further to a decreased compliance to your medical advice. What do you do next?
The parents get to know about your negligence, leading to extreme dissatisfaction in your medical care thus leading to them getting a Leave against medical advice issued and admitting their child under another doctor. You are now one patient poorer than yesterday
You scored 0 points.
Thank you for completing the case!
The child’s parents reported a urine dipstick of NIL for 3 consecutive days 4 weeks after administration of daily prednisone
Due to the therapy being inadequate, the patient returns to your OPD in 2 weeks with similar complaints and a urine dipstick of 3+ for the past 5 days. What would you do next??
The child kept on relapsing with more than 5 relapses in the initial 6 months. The parents got a second opinion from another pediatrician and got to know that the therapy prescribed by you to their child was extremely different from the treatment recommended by the guidelines. Dissapointed in your medical care, the parents file a medical negligence case against you and get their child admitted under a different pediatrician. Time to address your court summons!!
You scored 0 points.
Thank you for completing the case!
The child achieved remission successfully. However, 12 days after the completion of the child’s steroid regimen, the parents bring him back to your OPD saying that the urine dipstick had been showing 3+ for the past 6 days! What would be your next step?
The patient is responding pretty well to the therapy and has not relapsed. However, the parents noticed purplish striae on the child’s abdomen and a clearly noticeable central fat deposition and thus came to the OPD to ask for your advice.
The purplish striae and central obesity keep on worsening. The child develops hyperglycemia and hypertension leading to the full presentation of iatrogenic Cushing Syndrome. You started out treating a condition and instead created a worse one! The parents heavily disappointed in your medical care get their child discharged and admit him under a different pediatrician
You scored 0 points.
Thank you for completing the case!
The patient has been compliant to the treatment and has not relapsed. The purplish striae on the child’s abdomen have started to disappear and so has the central obesity. The patient has come for his first follow-up 2 weeks after being started on levamisole. What is the test to be done during the first follow-up after administration of levamisole?
You successfully managed to treat your patient! The patient led a comfortable life into adulthood and never relapsed again. However, if you did not get ANCA ordered, there might have been a chance that your patient would have developed ANCA vasculitis leading to devastating outcomes. Here, we have deducted points for the same but make sure to implement this during your practice!!
You scored 0 points.
Thank you for completing the case!
You were so close!! The patient was successfully treated for nephrotic syndrome and never relapsed. However, he developed severe neutropenia due to levamisole’s effects on the bone marrow and immune cells, this lead to recurrent infections in the child and thus worse prognostic outcomes. Do keep in mind to get ANCA panel and TLC done during follow-ups after levamisole therapy initiation.
You scored 0 points.
Thank you for completing the case!